In this video, Ketan K. Badani, MD, FRCS (Hon.) demonstrates the single-port, low-anterior approach to partial nephrectomy.
As surgeons made the shift from open surgery to laparoscopic and, more recently, robotic systems for partial nephrectomies, they switched from performing them retroperitoneally to transabdominally. Mount Sinai surgeon Ketan K. Badani, MD, FRCS (Hon.) is helping to reverse this trend through a new surgical approach that he has developed and refined over the past few years.
Dr. Badani’s approach combines single-port robotic technology with a low-anterior incision—a technique that enables him to resect any kidney tumor regardless of location retroperitoneally. This avoids entry into the abdominal space to access the kidney that would require mobilizing other organs and insufflating the abdomen.
This breakthrough has garnered considerable interest from his peers. Since he published the initial outcomes of the technique in 2022, Dr. Badani has presented lectures on the procedure and performed live demonstrations around the world. He has also welcomed visiting surgeons at Mount Sinai who are interested in observing and learning this technique.
“The low-anterior retroperitoneal approach is becoming synonymous with single-port robotic surgery,” says Dr. Badani, Professor of Urology and Director of the Kidney Cancer Center at the Icahn School of Medicine at Mount Sinai. “It is a real success story for surgical innovation that lowers invasiveness and improves the patient experience.”
Since he introduced the procedure in 2023, Dr. Badani has presented lectures and performed live demonstrations around the world.
According to Dr. Badani, the rate of adoption is outpacing that of robotic prostatectomy, which he helped pioneer. It is being performed at single-port health care systems nationwide and at centers in Australia, the European Union, South Korea, and Taiwan. Furthermore, data from a consortium of eight single-port centers hosted at Mount Sinai suggest that 100 percent of partial nephrectomy cases are being done retroperitoneally. This is particularly notable given that the percentage of retroperitoneal partial nephrectomies performed by multiport centers peaked at approximately 20 percent. Dr. Badani attributes that low uptake to two key factors: a general lack of retroperitoneal surgical training and the design of multiport systems, which does not easiliy facilitate a retroperitoneal approach.
“At Mount Sinai, we had to put some effort into making retroperitoneal partial nephrectomies work with our multiport system,” Dr. Badani says. “I shared the approach at educational symposia and live surgical demonstrations among other surgeons, but the muti-port retroperitoneal approach was never widely adopted.”
Dr. Badani believes the success of his low-anterior approach has been made possible both by the proliferation of single-port systems and the reproducibility of the technique, which he continues to refine.
There has been an evolution of the low-anterior access approach by reducing port sites to a single port incision only and maintaining a 100 percent retroperitoneal approach, as this technology is suited for small working spaces. Through increased comfort and experience, he has switched to a pure single-port procedure.
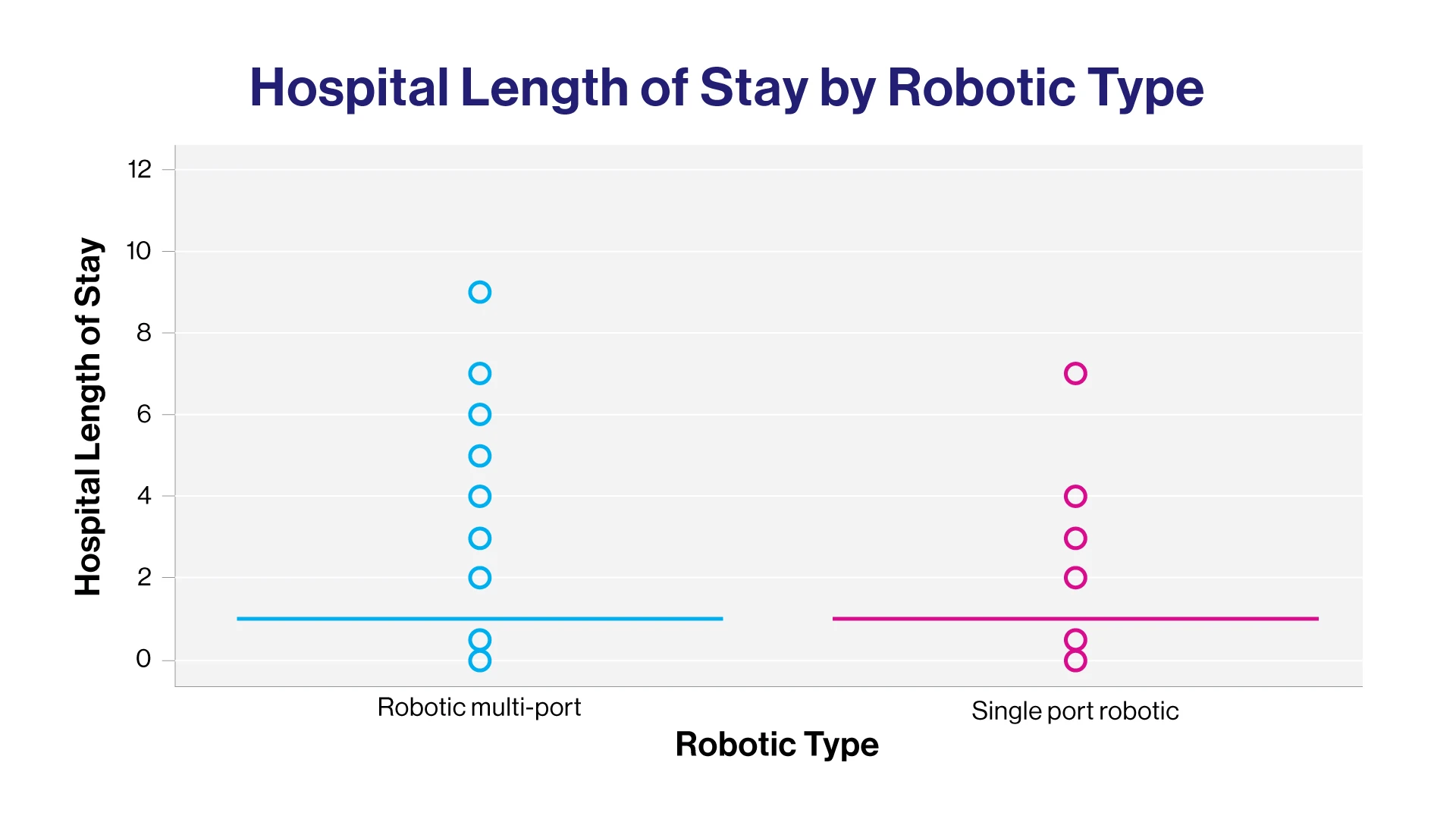
“Everything happens through a single 3.5 cm incision in this approach,” says Dr. Badani. Enhancements like this have enabled him to achieve significant reductions in total operative time (from more than two hours for multi-port to under one hour for single port) and length of stay. “We see a considerable advantage to keeping the patient supine for surgery as opposed to the traditional flank position. Not only is this much faster to start and complete surgery but avoids potential complications associated with placing a patient on their side in the flank position,” he says.
Although Dr. Badani performs the low-anterior, single-port partial nephrectomy as an in-patient procedure, the efficiencies he has achieved enable him to offer patients the option to go home following recovery. He says they are the largest group of urology surgery patients who choose to leave same day. This accomplishment was initially a focal point for assessing patient recovery, but physical activity has emerged as a more robust endpoint.
“For most multiport robotic kidney surgery, we advise four-to-six weeks before any heavy lifting, straining, or physical exercise other than walking or a light job, with the average time being 4.5 weeks,” he says.
“With the low-anterior approach, we had the same recommendation, but patients were telling us that they were in the gym or lifting on their own earlier. The average time to physical activity is 2.5 weeks so we see a full month of difference.”
Dr. Badani is pleased with these outcomes, and with the continued interest in his approach. He is looking to build on this momentum through further refinements of his technique, which will bring him closer to achieving his ultimate goal.
“I believe we should stay out of the abdomen for all kidney surgery given the degree of internal trauma associated with that approach,” he says. “Ninety percent of surgery is still happening that way, so we have a long way to go. But I hope that, through my efforts, no one will enter the abdomen to do a partial nephrectomy anymore.”