
For years, Mount Sinai urologists have been administering radiation and hormone-based therapies to treat patients who present with aggressive prostate cancer. But the battle is about to get more personal with a new clinical trial that is exploring the potential of a personalized vaccine approach.
The phase 1, open-label, single-center, proof-of-concept study is assessing the safety and tolerability of administering a PGV001-based multi-peptide vaccine—a fully personalized therapeutic vaccine directed toward mutation-derived tumor antigens—in combination with CDX-301, a potent hematopoietic cytokine.
The study among patients with a history of aggressive cancer in the tumor-free adjuvant setting is being led by Ash Tewari, MBBS, MCh, FRCS (Hon.), Professor and System Chair, Milton and Carroll Petrie Department of Urology, and Director of the Center of Excellence for Prostate Cancer at The Tisch Cancer Institute at the Icahn School of Medicine at Mount Sinai.
“Personalized vaccine therapy has been studied and has been found to be very safe and effective in achieving tumor regression in other cancers, but this approach has not previously been tested for prostate cancer,” says Sujit S. Nair, PhD, Assistant Professor and Director of GU Immunotherapy Research at the Department of Urology at Icahn Mount Sinai. “Our extensive experience in treating prostate cancer suggests this could be a viable approach because we are able to identify new antigens in the prostate. Thus, we believe we will find patients who will benefit from this treatment.”
Sujit S. Nair, PhD, Assistant Professor and Director of GU Immunotherapy Research at the Department of Urology at the Icahn School of Medicine at Mount Sinai
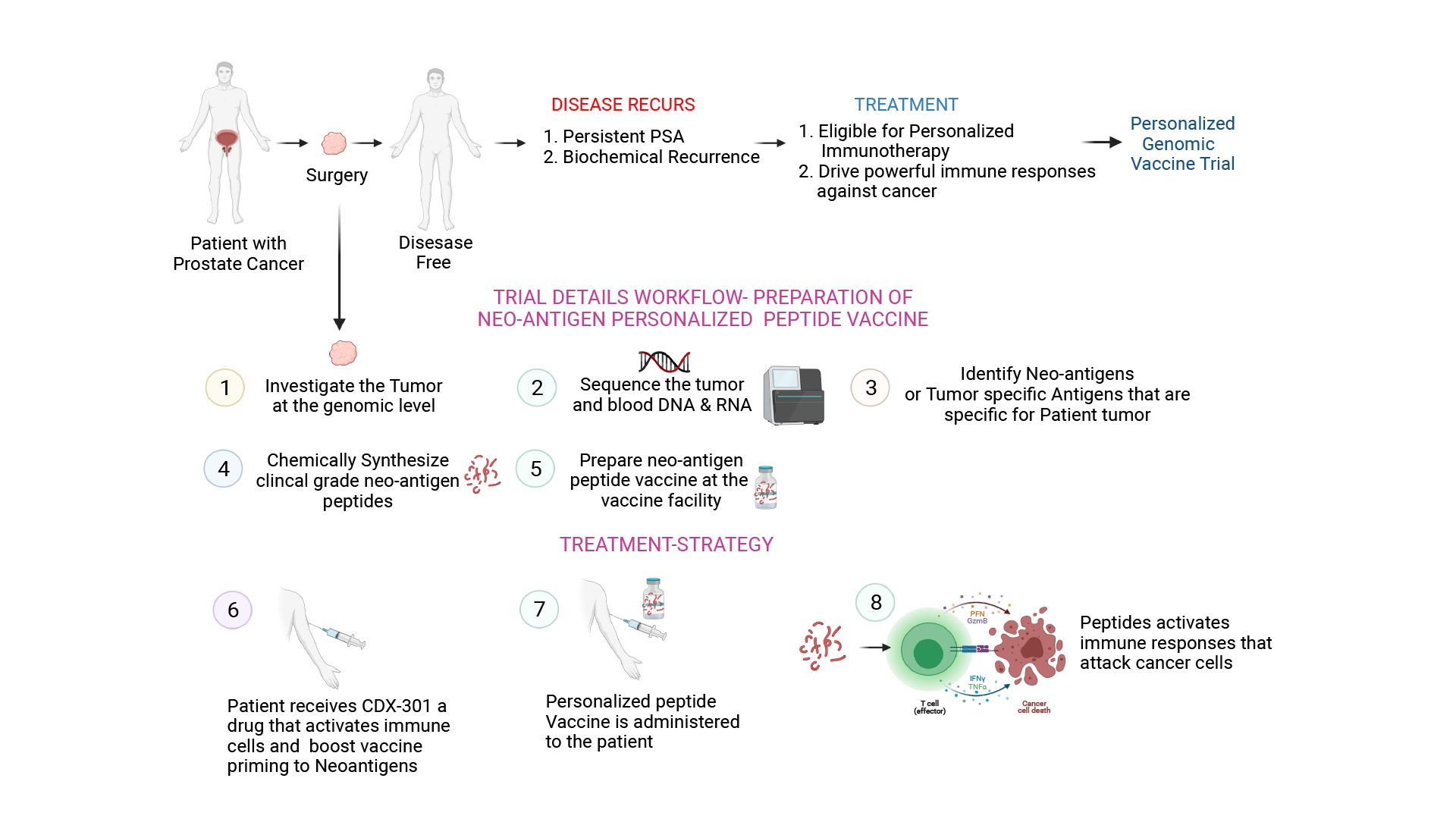
The criteria for participant eligibility include a histologically proven diagnosis of adenocarcinoma of prostate; elevated or persistent prostate-specific antigen (PSA) post-surgery; biochemical recurrence (defined as PSA value ≥ 0.2ng/ml) or an estimated risk of biochemical recurrence within five years of 30 percent or more as assessed by Decipher report; completion of radical prostatectomy and additional standard of care therapies, and be clinically tumor free; and ability to provide the necessary tissue sample for sequencing.
Each potential candidate will undergo extensive screening and genomic sequencing to assess the presence of mutation-derived tumor antigens—which will enable the development of the personalized vaccine. Mount Sinai researchers will conduct blood sequencing to determine the patients’ germline mutations and then conduct tumor sample sequencing to determine the total mutations.
The differences between the two mutations are the mutation-derived tumor antigens. The researchers will then analyze these acquired mutations to determine whether they change the protein function and how many of these qualify as new proteins with a high affinity for major histocompatibility complex (MHC) binding.
“If the proteins have a high affinity for MHC binding, then the cancer has used the proteins to somehow escape immune system surveillance,” Dr. Nair says. “But these new mutations can be presented by MHC, which means they can be presented to the immune cells. Using that logic, we can use these mutations to design peptides that correspond to these antigenic sequences and then send the peptide sequences to JPT Peptide Technologies, which will design and produce clinical-grade peptides that we can use to vaccinate study participants.”
The personalized genomic vaccine will be prepared within the Vaccine and Cell Therapy Laboratory (VCTL) in a Good Manufacturing Practices-certified environment under the guidance of Nina Bhardwaj, MD, PhD, Director of the Immunotherapy Program and the Ward-Coleman Chair in Cancer Research at The Tisch Cancer Institute at Mount Sinai, and Professor of Medicine (Hematology and Medical Oncology) and Urology at Icahn Mount Sinai, who is the Co-Principal Investigator. In the first stage of the trial, three patients will be administered a personalized genomic vaccine at Mount Sinai’s Ruttenberg Treatment Center.
Once Dr. Tewari and his colleagues have confirmed the safety of this therapeutic approach, a second subset of three patients will receive both the genomic vaccine and CDX-301. Based on the safety outcomes, an expanded cohort of 25 patients will receive the combined therapeutic approach, which will consist of 10 doses of the genomic vaccine (days 1, 3, 8, 15, 22, 36, 50, 78, 106, and 183) and two doses of CDX-301—one administered one week prior to the first dose of the vaccine, and one administered prior to the sixth dose.
Mount Sinai researchers will conduct blood collection among participants both prior to and during the study to assess changes in PSA levels, among other indicators, to assess the safety and clinical benefits of this approach.
Candidate identification is underway, and Dr. Nair says the team is looking at patients who have undergone surgery with Dr. Tewari, have available tissue, and are willing to enroll in the trial as potential candidates.
“If we are able to confirm that this therapeutic approach is safe and achieve clinical benefits, that will open the door to conduct a phase 2 study with a larger cohort of patients and potentially bring us one step closer to a new treatment for patients with aggressive prostate cancer,” he says.
A phase 1, open-label, single-center, proof-of-concept study will assess the safety and tolerability of administering a PGV001-based multi-peptide vaccine—a fully personalized therapeutic vaccine directed toward mutation-derived tumor antigens—in combination with CDX-301, a potent hematopoietic cytokine.