A brain-computer interface (BCI) is a type of technology that records brain activity, interprets that brain activity, and then uses that interpretation to control an external device, says David Putrino, PhD, Director of Rehabilitation Innovation for the Mount Sinai Health System. “Depending on the type of BCI technology, that device might be as complex as a robotic arm or as simple as a mouse pointer, but the general idea is the person can think and the technology responds.”
Dr. Putrino is a Principal Investigator of the COMMAND trial, which is testing a type of BCI called the Stentrode, built on an endovascular electrode array manufactured by New York-based Synchron. The study is funded by the National Institutes of Health’s Brain Research Through Advancing Innovative Neurotechnologies (BRAIN) Initiative.
“I think this is a very exciting project, with the potential to change the level of independence that is possible for people with severe paralysis.”
David Putrino, PhD
Until now, BCI technologies have required open-brain surgery for implantation, where the skull is cut open and an electrode placed directly into the brain tissue, with a visible socket coming out of the person’s head. The procedure involves risk, and also eventual loss of signal over time due to the buildup of scar tissue.
In contrast, the Stentrode—which received a Breakthrough Device designation by the U.S. Food and Drug Administration in August 2020—is minimally invasive and involves the same stenting procedure that vascular surgeons commonly perform to treat stroke. In this case, the stent is snaked via the patient’s jugular vein into the superior sagittal sinus, the large vein located between the two brain hemispheres. The stent is then opened up so that the electrodes are placed adjacent to the primary motor cortex.

The endovascular implant to be placed in a vein alongside the motor cortex, which generates any signal related to movement.

The receiver device that would be implanted in the chest to transmit the neural signals to a decoder.
Once in place, the electrodes record all electrical activity from the brain. The surgeon plugs the wire into a pacemaker-like device that is implanted just below the skin in the person’s upper chest. An external device is then placed over the chest, which receives the brain activity from the internal device and uses Bluetooth to record the electrical activity coming from the electrode. “It’s a very well-designed technology that overcomes a lot of the limitations of the previous BCI technologies that have been trialed in the past,” Dr. Putrino says.
Over time, the system learns to map signals from the patient’s brain to specific computer commands, allowing for cognitive control of a digital device to perform tasks such as computerized speech, environmental control (e.g., turning lights on and off), personal banking, digitally signing documents, or engaging in social media.
“Ultimately, we aim to empower participants such that they can use this technology to achieve full independent control of a personal computer. Through a combination of very clever sensor technology and equally clever machine learning algorithms, we can decode a participant’s cognitive impulses and map them onto specific commands that control a laptop cursor,” Dr. Putrino says.

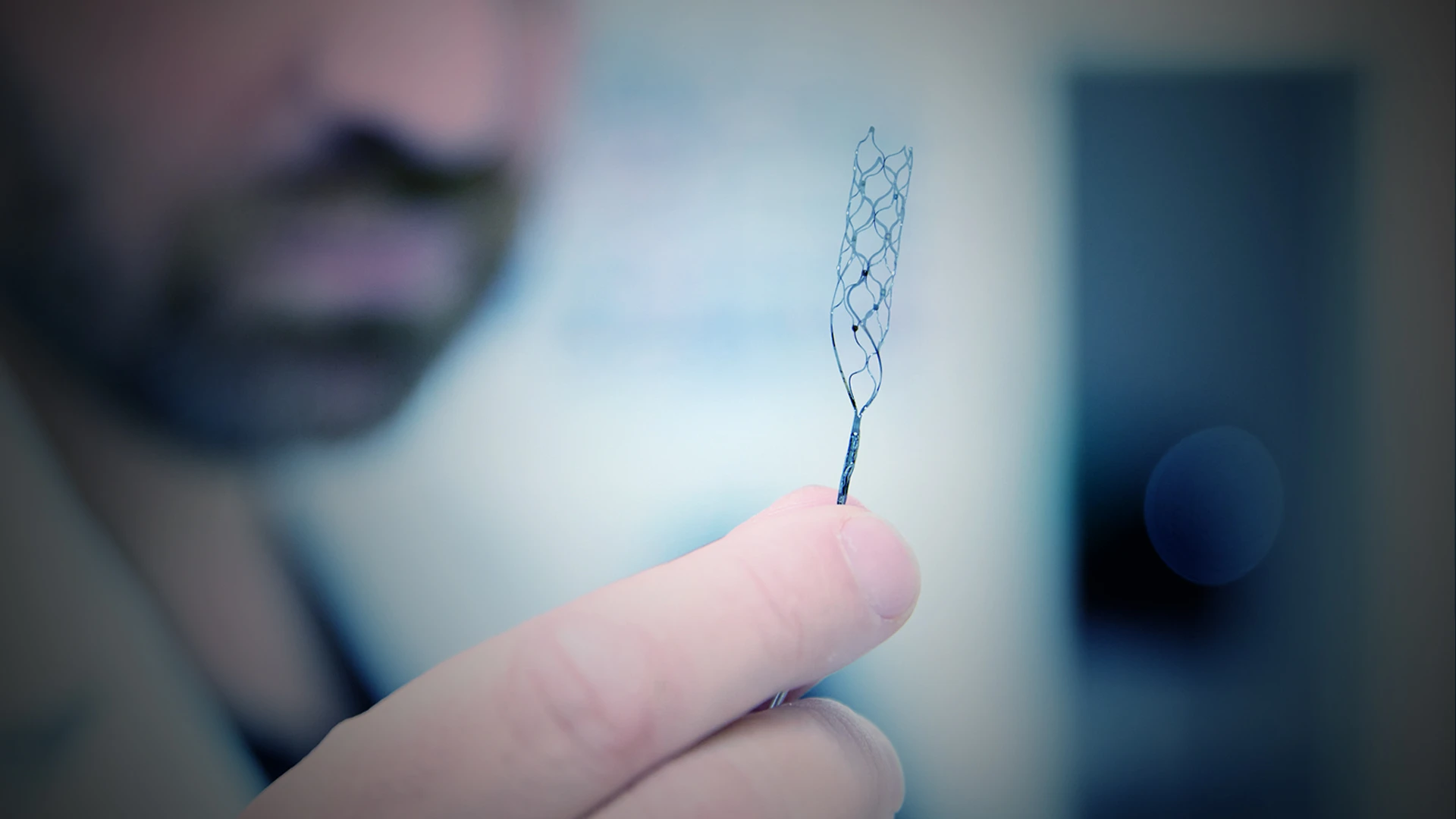
David Putrino, PhD, demonstrating to Nick Greiner, Australian Consul-General, New York, what the Stentrode endovascular implant looks like and how it'd work for people living with paralysis.
Mount Sinai neurovascular surgeon Shahram Majidi, MD, performed the first Stentrode implant in July 2022 on the study’s first participant, who was completely paralyzed due to amyotrophic lateral sclerosis. Unlike previous BCI systems where all testing is done in a laboratory, the participant was able to go home after just two days with the device live. Additional potential study participants have been screened, including those with severe paralysis due to neurological conditions such as high-level spinal cord injuries and stroke.
Previously, four Australian patients who received the implants all achieved independent home use within six months. “What we see here is an impressive push forward in the ability of a minimally invasive BCI technology to make a very real functional difference in a user’s life in a way we’ve never seen with other invasive BCI technologies,” says Dr. Putrino.
Although it will be some time before the system becomes commercially available, Dr. Putrino predicts the cost and insurance coverage will likely be in the ballpark of current augmentative technologies on the market. After all, insurers already cover many interventions that help patients communicate, such as technologies that tell a caregiver that a patient has a urinary tract infection coming on or is having trouble breathing.
“These are things that people living with severe paralysis routinely need to communicate,” Dr. Putrino says. “If they can do so easily, it may mean faster access to antibiotics, to a more intensive care level where maybe they can avoid hospitalization or getting sick in the first place, thereby deferring a lot of long-term care costs.”
Featured

David Putrino, PhD
Director of Rehabilitation Innovation, and Professor of Rehabilitation and Human Performance