
A multidisciplinary team successfully performed the Mount Sinai Health System’s first ovarian tissue cryopreservation procedure, removing ovarian tissue and saving it for future reimplantation, giving the hope of future children to a young woman undergoing cancer treatment. “After several years of laying the groundwork for ovarian cryopreservation, the first opportunity presented itself quickly when we met this patient,” says Kellie Woodfield, MD, who coordinated the procedure. Dr. Woodfield is Assistant Professor of Obstetrics, Gynecology, and Reproductive Sciences, and Pediatrics at the Icahn School of Medicine at Mount Sinai.
The young woman was pregnant with her first child when she was diagnosed with perianal rhabdomyosarcoma, a rare and often aggressive form of cancer that required urgent treatment. The necessary chemotherapy regimen, however, was unsafe for the fetus—and toxic to the ovaries and likely to impair future fertility. To expedite the patient’s cancer treatment, her medical team planned for a Cesarean birth at 31 weeks of gestation. Dr. Woodfield and a team of collaborators arranged to retrieve the ovarian tissue for cryopreservation during the same procedure.
The C-birth was performed by maternal-fetal medicine specialist Jessica Spiegelman, MD, Assistant Professor of Obstetrics, Gynecology, and Reproductive Sciences at the Icahn School of Medicine. Katherine Halper, MD, assisted in the surgery and performed the oophorectomy. Other departments also played key roles, including pediatric urology, reproductive endocrinology, maternal-fetal medicine, and more. Nonclinical teams also played a crucial role, Dr. Woodfield says, including mailroom staff members, who pitched in to ensure the speedy retrieval of the transport medium needed to ship the ovarian tissue to the University of Pittsburgh Medical Center, the national leader in processing ovarian tissue for cryopreservation. “It was a Herculean effort from a large and multidisciplinary team who pulled out all the stops to give this patient a chance at future pregnancies,” Dr. Woodfield says.
Egg freezing, the well-established fertility preservation method, is not an option for those who have not gone through puberty or who are not emotionally mature enough to undergo the lengthy and invasive procedure. The egg-retrieval process can take several months, so egg freezing is also not suitable for patients who require urgent cancer treatment. For such patients, ovarian cryopreservation can be an appropriate alternative.
“In a different place and time, this would have been her only baby. Now there’s hope that wasn’t there before.”
Kellie Woodfield, MD
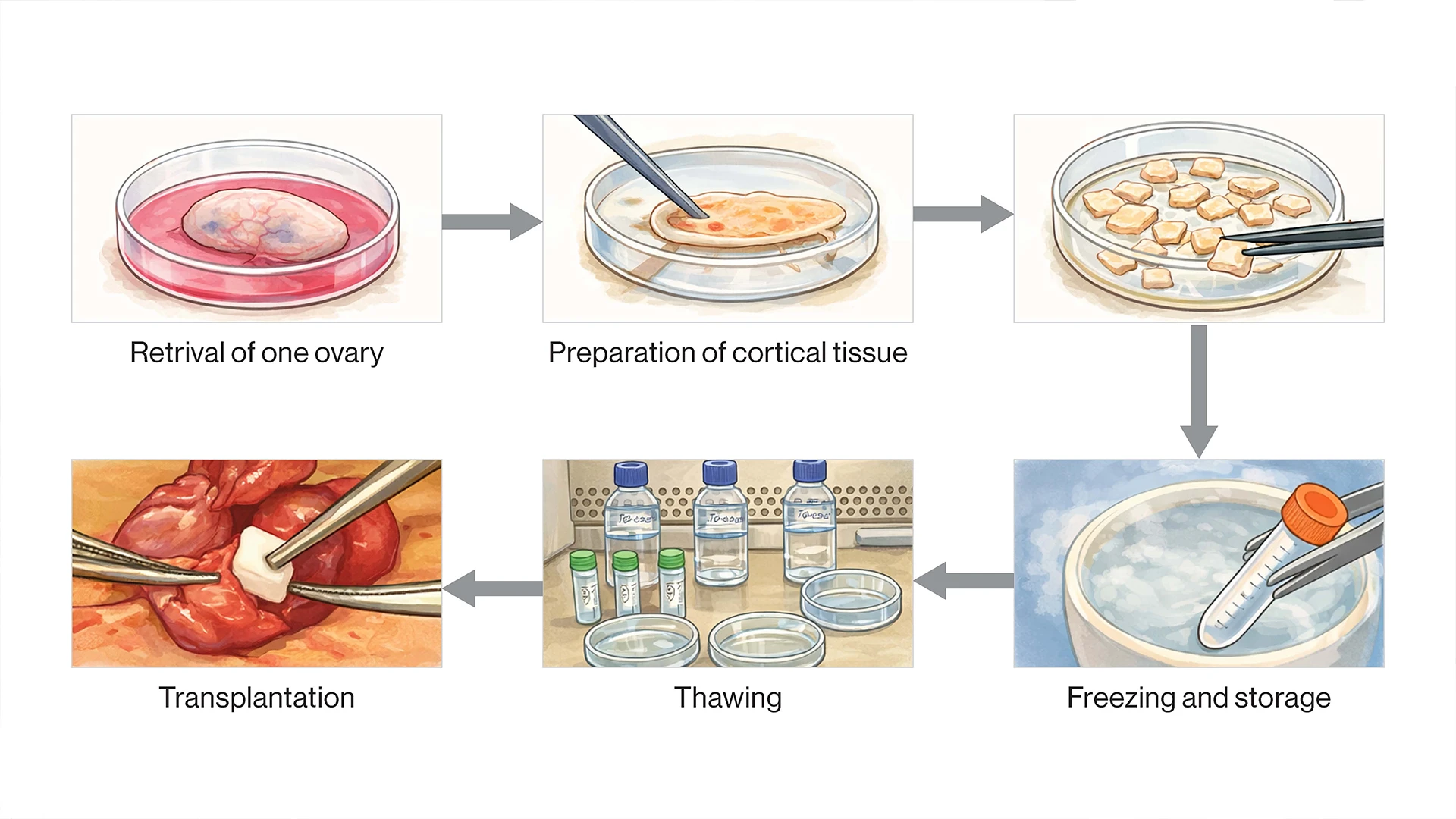
In ovarian cryopreservation, the ovary is surgically removed from the body. The cortex of the ovary, which contains the oocytes, is separated from the rest of ovary and prepared for freezing. The ovarian tissue is frozen and stored for later use. When the ovarian tissue is ready to be implanted back into the body, it is thawed, then surgically transplanted into the pelvis.
Yding Andersen C, Mamsen LS, Kristensen SG. FERTILITY PRESERVATION: Freezing of ovarian tissue and clinical opportunities. Reproduction. 2019 Nov;158(5):F27-F34. doi: 10.1530/REP-18-0635.
In the future, when a patient is ready to pursue pregnancy, cryopreserved ovarian tissue is reimplanted back into the pelvis, where it resumes producing hormones and releasing eggs. Because the procedure is relatively new, data on success rates are limited. But the best available data suggest that about half of patients can conceive spontaneously after ovarian tissue reimplantation, while others can conceive with help from fertility treatments. “We’re so glad to offer this option to our patients, but it is still an expensive procedure that is cost-prohibitive for a lot of people,” Dr. Woodfield says. “We’re hopeful that as the program grows, we can decrease barriers to access.”
With the addition of ovarian cryopreservation, Mount Sinai now offers a comprehensive fertility preservation program, which includes egg freezing, ovarian tissue cryopreservation, sperm freezing, and testicular tissue cryopreservation. “Patients and providers don’t always realize these options are available to preserve future fertility,” says Neha Malhotra, MD, FACS, FAAP, Associate Professor of Urology at the Icahn School of Medicine, who heads the fertility preservation program. “Anyone undergoing cancer treatment that could affect their fertility should be referred for a fertility-preservation consultation.”
The procedure is a testament not only to advances in reproductive medicine but also in oncology. “For so long, so much of cancer care focused on survival. Now that we can assume many of these patients will survive, we can think long-term about their quality of life into the future,” Dr. Woodfield says. “This is one more step toward changing the narrative around cancer care.”
The ovarian cryopreservation patient delivered a healthy baby at 31 weeks. “The birth was a beautiful experience. There were a lot of emotions in the room and so much gratitude,” Dr. Woodfield says. The patient’s cancer treatment is progressing as planned, and she and her child are doing well, she adds. “In a different place and time, this would have been her only baby. Now there’s hope that wasn’t there before.”