When medications did not effectively treat her pain and her TN symptoms progressively worsened, Dr. Miller collaborated with Joshua B. Bederson, MD, to determine that surgery was the most effective course of treatment.
In this narrated video case presentation, Dr. Miller and Dr. Bederson demonstrate how surgical intervention for TN can provide durable, long-term relief in appropriately selected MS patients.
Dr. Miller is the Medical Director of the Corinne Goldsmith Dickinson Center for Multiple Sclerosis and Professor of Neurology at the Icahn School of Medicine at Mount Sinai. Dr. Bederson is the Leonard I. Malis, MD/Corinne and Joseph Graber Professor of Neurosurgery, and Chair of the Department of Neurosurgery for the Mount Sinai Health System.
“At the point I first saw her, she had moderate lower extremity weakness and obvious difficulty with her gait,” recalls Dr. Miller. “The MRIs at that time were characteristic for MS. She had multiple T2 hyperintense lesions, including several lesions that abutted the lateral ventricles, which are characteristic locations for MS lesions. She also had spinal cord lesions, including a lesion at T2. She was relatively stable until 2017 when she developed severe stabbing facial pain that was consistent with TN.”
The patient was referred to Dr. Bederson, who saw her in 2018. “She described the classic symptoms of left V2 and V3 distributions,” says Dr. Bederson. “The MRI showed a loop of the superior cerebellar artery that was possibly compressing the left trigeminal nerve. The nerve was also seen to be diminutive, possibly due to effects of the MS. My recommendation was for posterior fossa exploration and possible microvascular decompression.”
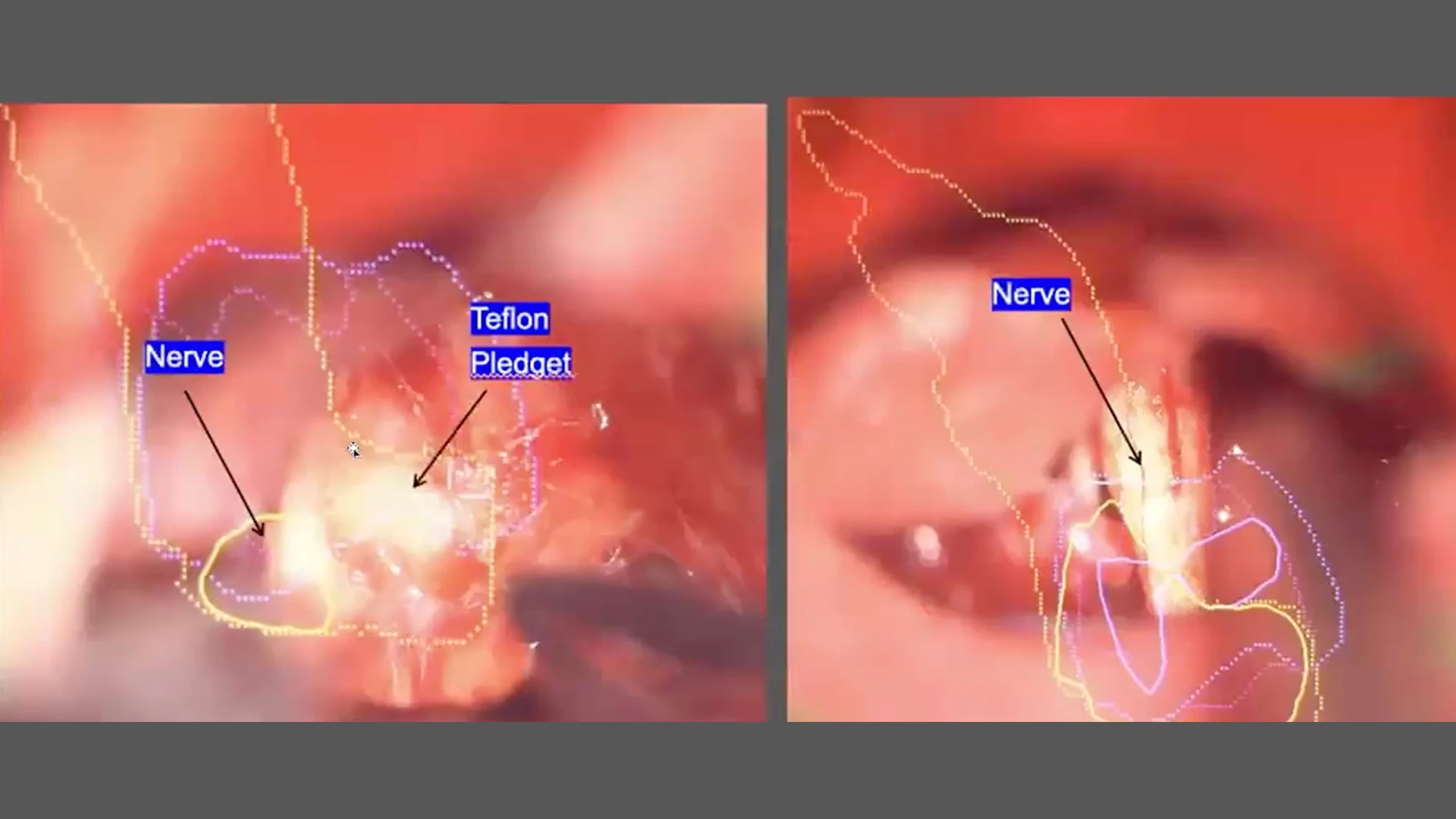
Adds Dr. Bederson, “What I have found in cases like this is that with moving, massaging, and gently compressing the nerve, we can sometimes eliminate the trigeminal neuralgia that's caused by the atrophy. In addition, we displaced blood vessels away from the nerve and placed a Teflon pledget.”
Surgical intervention for trigeminal neuralgia can provide durable, long-term relief in appropriately selected multiple sclerosis patients.
The patient was entirely pain-free for one year before the TN recurred. “In these cases,” says Dr. Bederson, “it's often due to development of scar tissue around the nerve, and I have found that a re-operation has a similar success rate to the initial operation. The second operation consisted of resecting the scar tissue and freeing up the nerve as far as we could see it from distal all the way to proximal where it enters the brain stem. To my delight, she awakened without any trigeminal neuralgia.”
Dr. Miller concludes: "I've now seen her five years following her latest vascular loop surgery and she has been completely pain-free.”
Watch the video:
After medications were unsuccessful, a Mount Sinai neurologist and neurosurgeon collaborated and treated a patient with multiple sclerosis and debilitating trigeminal neuralgia using targeted surgery to relieve nerve compression and restore long-term, pain-free function.