
Managing single-sided hearing loss among patients with vestibular schwannomas, also known as acoustic neuromas, has long posed considerable challenges, specifically the relative lack of options for improving or preserving hearing. The challenge now, according to Mount Sinai’s Maura Cosetti, MD, is recommending the right option.
“There has been an explosion of options, but there is not necessarily one clear solution,” explains Dr. Cosetti, Director of the Ear Institute of the New York Eye and Ear Infirmary of Mount Sinai and the Cochlear Implant Program of the Mount Sinai Health System. “It is a very complicated topic that requires the interaction of many specialists—otolaryngologists, neurosurgeons, and audiologists—in making a decision.”
Step One: Identifying the Best Approach
The complicated decision process often starts with determining the optimal approach for treating these benign tumors among patients: observation, radiation, or surgery. Each has an attendant risk for further hearing loss—surgery and radiation due to potential damage to the cochlear nerve and observation due to lack of action. The approach Dr. Cosetti and her colleagues take is determined based on several factors. These include the location and size of the tumor as well as the patient’s age, symptoms, and preferences.
“In an ideal world, we would resect the tumor and the patient’s hearing would be preserved, but that may not be possible based on the tumor’s size and location or the level of hearing loss the patient has already experienced,” Dr. Cosetti says.
Step Two: Preserving or Improving the Patient’s Hearing
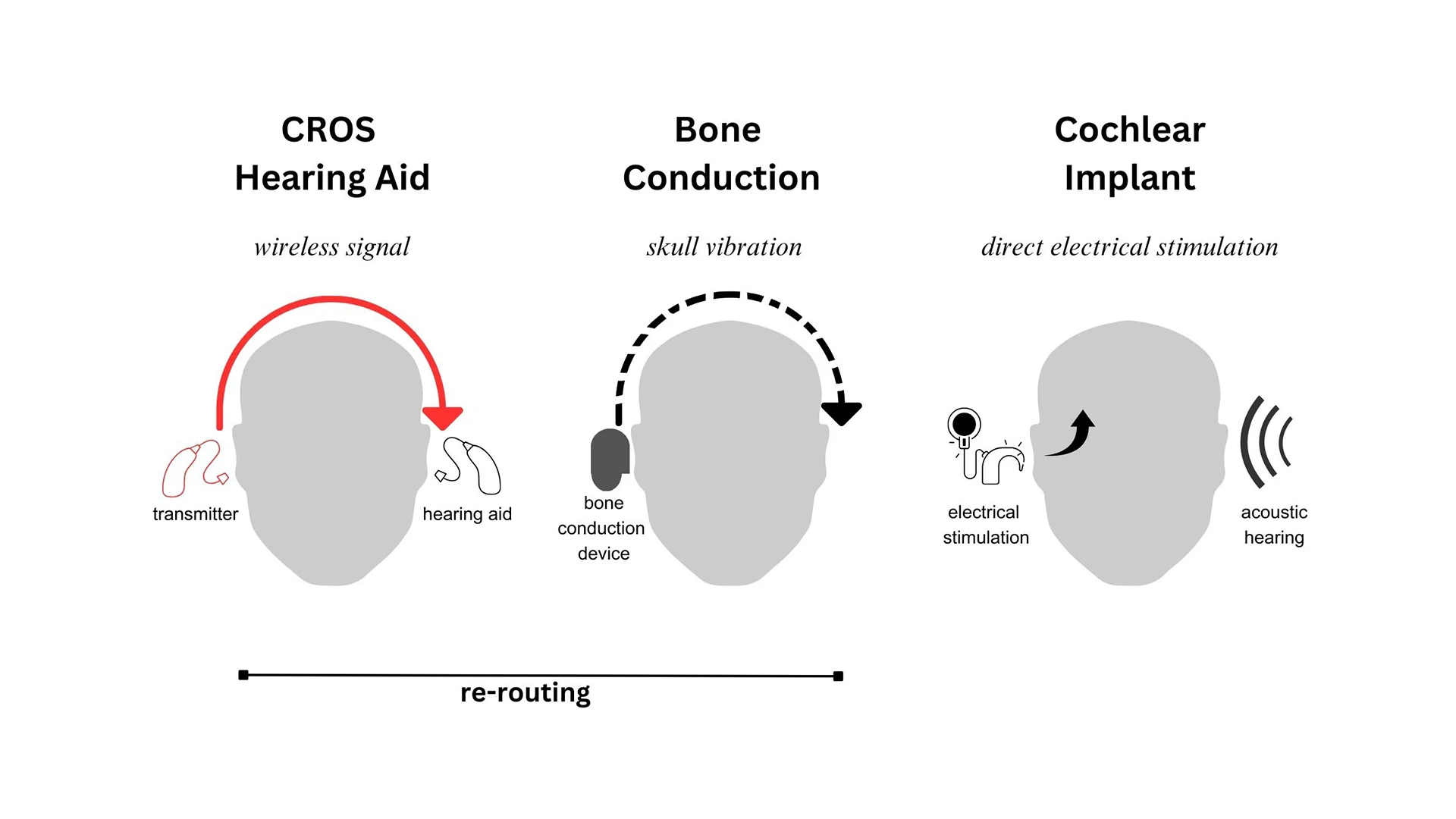
Once a determination is made as to treatment, the focus shifts to preserving or treating the patient’s hearing. Many of the same factors are considered in making recommendations, in particular, the degree of hearing loss the patient has experienced. For patients who retain some hearing, Dr. Cosetti typically recommends a hearing aid. For those who have experienced complete hearing loss and who do not have an intact cochlear nerve, there are a couple of options. One is a contralateral routing of signal (CROS) hearing aid. This system uses a microphone and transmitter to send sound from the patient’s non-hearing ear to the hearing side. Although it can be effective, Dr. Cosetti notes that it does not aid in localizing sound and some patients are reluctant to use it as it requires them to use a hearing aid in their good ear. For these patients, Dr. Cosetti typically recommends a bone conduction hearing aid. It sends sound wirelessly from the side that is experiencing deafness to the good ear using the vibrations of the skull without the requirement for a hearing aid. Moreover, there are wearable options for patients who are averse to surgical implants.
“Some of the bone conduction options are nicer for patients’ quality of life,” Dr. Cosetti says. “For one, the technology has evolved so they are not only more cosmetically appealing, but also the surgical bone conduction systems are now MRI compatible. That is invaluable because patients with vestibular schwannomas need to undergo MRIs to ensure the tumor has not grown back.”
Another Option for Some Patients: Cochlear Implantation
Although it has been widely used for other indications of single-sided deafness, cochlear implantation has only recently been offered to patients presenting with vestibular schwannomas. That, Dr. Cosetti says, was the result of prevailing medical dogma that the position of the schwannoma rendered the implantation option ineffective. Moreover, the Food and Drug Administration has not approved cochlear implantation for vestibular schwannomas, and some insurers will not cover it for this indication.
“We have found it is possible to do an implant that benefits patients so long as the cochlear nerve is intact,” says Dr. Cosetti. “Whether that is a patient whose nerve was preserved during surgery or someone with stable, long-standing tumors and poor hearing, a cochlear implant is a very good option for them.”
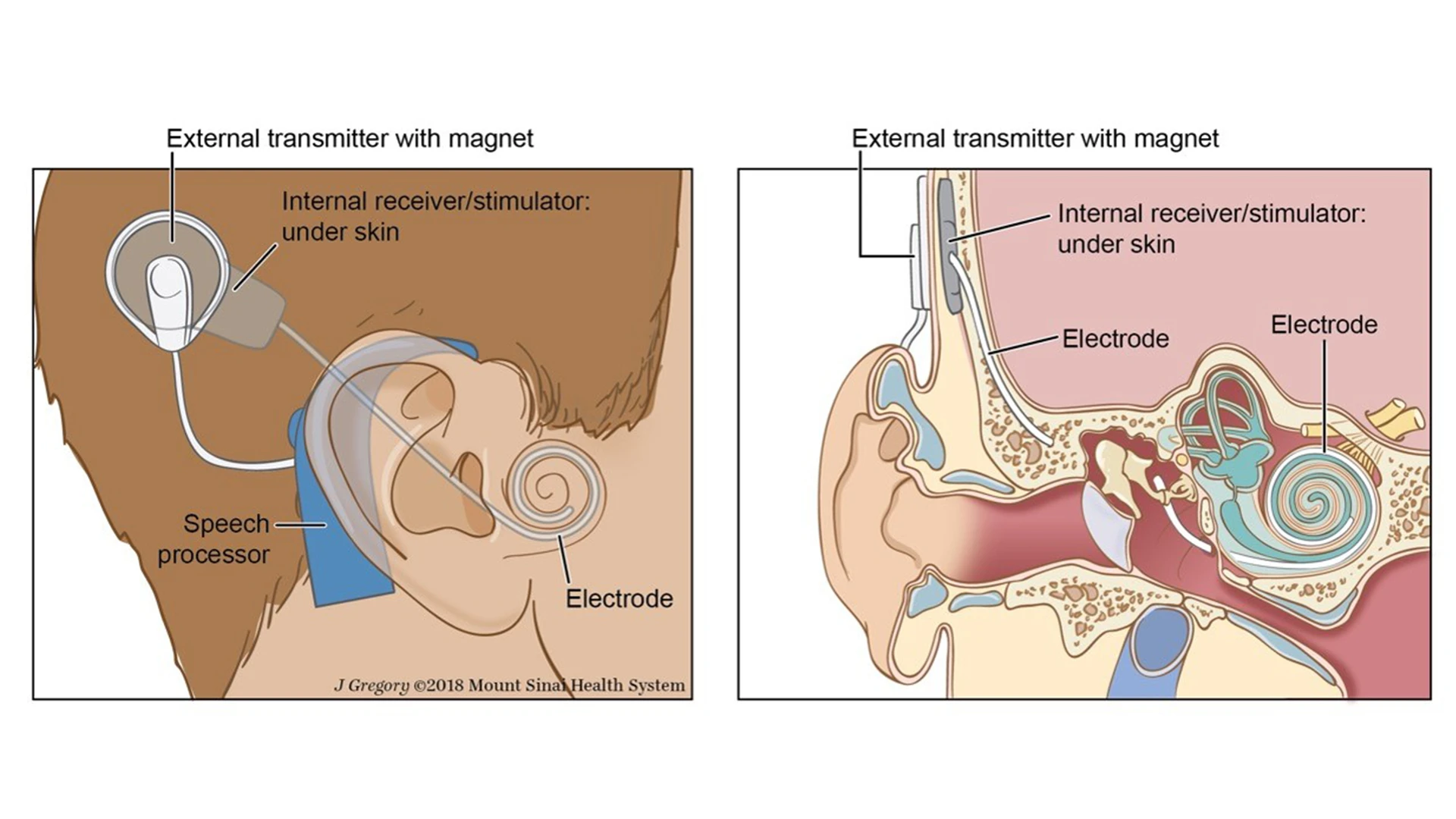
Cochlear implantation
Extrapolated data on single-sided deafness from a non-acoustic neuroma suggests patients experience dramatic improvements in quality of life, ability to localize sound, and ability to understand speech in noisy environments among patients who have undergone cochlear implantation. Dr. Cosetti’s goal now is to better understand the benefits of implantation from the perspective of patients with vestibular schwannoma-related hearing loss.
“We know that it seems to be better when compared against bone conduction devices,” she adds, “but we do not know how much better, and we do not know if it is the same as with patients with a non-vestibular schwannoma. That is what we need to look at now.”
Featured
Maura K. Cosetti, MD
Assistant Professor of Otolaryngology—Head and Neck Surgery