For too long, hair loss—or alopecia as it’s known clinically—was considered to be a cosmetic condition, unfortunate but perhaps not urgent. And the treatments, too, have been few and far between, either less than fully effective or not safe for the long term.

Emma Guttman, MD, PhD, left, leads the research team at the Alopecia Center of Excellence, where new studies are cause for hope for patients.
All of that is now changing, thanks to the innovative efforts of Emma Guttman-Yassky, MD, PhD, and Benjamin Ungar, MD, who head up the research team at the Alopecia Center of Excellence at Mount Sinai. Dr. Ungar, Director of the Center, is keenly interested in the psychosocial impact of alopecia—and, also, in raising awareness, including among insurers, of the toll the condition can take on patients and their families. “Until recently, the enormous psychological effects of the disease were underappreciated,” says Dr. Ungar. “For men, in particular, it’s easy to think that baldness is no big deal. But I’ve seen many patients, both women and men, who tell me they look in the mirror and don’t recognize themselves, that they don’t feel they have anything to live for.”
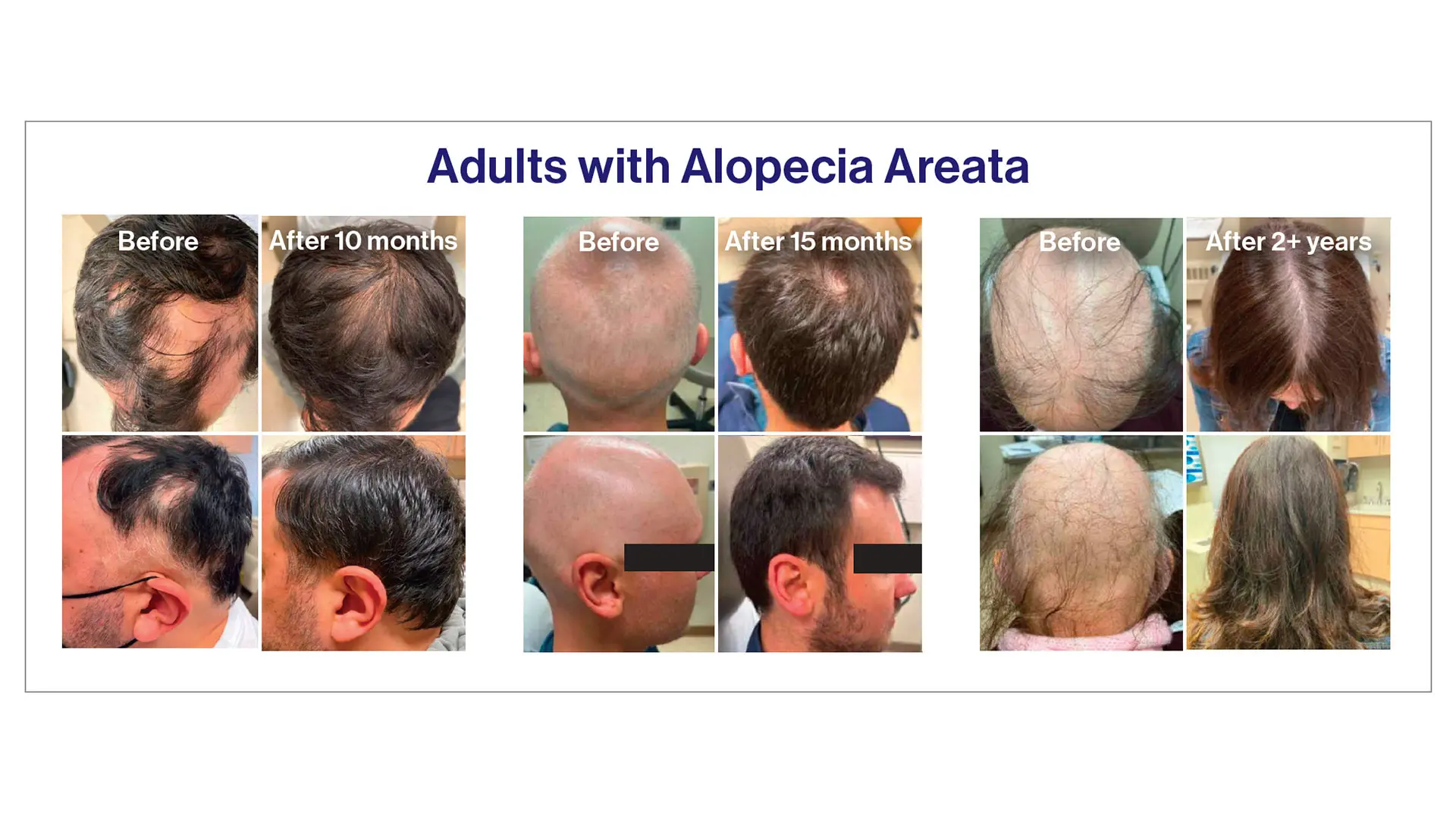
Now, exciting new studies at the Alopecia Center are cause for hope for these patients, shedding light on the underlying processes that lead to alopecia and pointing to new and safer therapies. That’s the case for alopecia areata, an autoimmune inflammatory skin disease affecting more than 6.7 million Americans, which can cause patchy to total hair loss, including of the eyebrows and eyelashes.
New Treatments Have Brought Progress— With Limits
Until three years ago, the only available therapies for adults and children with alopecia areata were painful steroid injections (as many as 100 injections per treatment) or broad-based immunosuppressant medications, including systemic steroids, methotrexate, cyclosporin, and treatments used to tamp down immunity in organ transplant patients, which all have potentially negative side effects, according to Dr. Ungar. That changed when three oral immune-modulating medications known as Janus kinase (JAK) inhibitors were approved to treat alopecia areata.
But while that has been a tremendous step forward, not everyone is a candidate for these medications, which come with a “black box” warning and are not approved for use in children under age 12. “Clearly, there is still a huge treatment gap,” says Dr. Ungar.
A Touch of Serendipity
Then, in 2015, Dr. Guttman noticed something interesting while studying patients with atopic dermatitis who were being treated with another immune-modulating therapy known as dupilumab. “You could say that I got interested in alopecia areata through the back door, while focusing on atopic dermatitis,” says Dr. Guttman, Waldman Professor of Dermatology and Immunology and System Chair of the Kimberly and Eric J. Waldman Department of Dermatology at the Icahn School of Medicine at Mount Sinai. “What I noticed is that some of my patients with atopic dermatitis who also happened to have alopecia areata and were being treated with the specific anti-type 2 immune cells monoclonal antibody drug dupilumab, began to grow hair,” she recalls.
This was a major development given that dupilumab had an extensive safety profile, so much so that it is used to effectively treat infants and young children with atopic dermatitis—and adults, too—with very few side effects. But the Dr. Guttman discovery also flew in the face of conventional wisdom in terms of what was driving the immune processes of alopecia areata versus atopic dermatitis.
Specifically, prior to Dr. Guttman’s discovery, atopic dermatitis and alopecia areata were thought to be activated by different poles of the immune system, the former by so-called type 2 immune cells and the latter by type 1 cells. Logically, that meant the same immune-targeting medication should not work to ease both conditions.
A Startling Connection Between Alopecia and Eczema and Other Allergic Conditions
Dr. Guttman and the team set out to get to the bottom of the conundrum. “We began looking at the literature on patients with alopecia areata and discovered that there had been quite a few observations that these patients also had a high degree of atopy—meaning a family or personal history of asthma, allergies, eczema, and high immunoglobulin E (IgE)—all of which are activated by type 2 immune cells,” she explains. “Nobody had linked this together before.” The implications were evident to Dr. Guttman: First, that alopecia areata was also characterized by type 2 immune activation, just like many allergic conditions, eczema included. And second, that dupilumab, the same immune- modulating medication currently being used to treat people of all ages with moderate to severe atopic dermatitis, might also be effective in regrowing hair in patients with alopecia areata.
Dr. Ungar explains: “Unlike JAK inhibitors, which act more broadly on the immune system and block several immune pathways, dupilumab is very targeted. Rather than blocking large swaths of the immune system, it targets only the IL-4 receptor (blocking IL-4 and IL-13), which is involved in allergic inflammation,” he explains. “That’s what makes it safer.”
And indeed, two subsequent studies of patients with alopecia areata conducted at the Center found that people who also had allergic atopy (typically more than 50 percent of alopecia areata patients) began to regrow their hair. “We showed that when alopecia areata is a multifactorial disease co-existing with atopy, type 2 immunity does play a role, which opens the door to treatment with dupilumab,” says Dr. Guttman.
Dr. Guttman believes that dupilumab may also be beneficial for certain non-dermatological conditions driven by inflammation, including COVID-19 responses. “During the pandemic, we discovered that some of our patients who were taking dupilumab who should have been susceptible to severe COVID-19 didn’t get sick,” she says. “I’m thinking of one patient with eczema and alopecia areata who was obese and had diabetes and who, unfortunately, had several siblings who died from the virus—but he ended up not getting sick. It turns out that dupilumab seems to reduce the manifestations of COVID-19, too.”
Adds Dr. Ungar: “The idea that dupilumab might work for alopecia areata was on no one’s radar, but through Dr. Guttman’s insights, we have been able to move things forward. We are quite excited about the potential.”
Benjamin Ungar, MD, right, is the Director of the Alopecia Center, and is shown with Yeriel Estrada, Clinical Research Program Director.
Progress for Scarring Alopecia
Making these kinds of connections is all in a day’s work for Dr. Guttman, who is now turning her attention to three types of so-called scarring alopecia known as frontal fibrosing alopecia (FFA), which is increasing in prevalence, as well as lichen planopilaris and central centrifugal cicatricial alopecia (CCCA). “The first two of these most commonly occur in women, often starting when they are in their late forties, and can cause a receding hairline, along with redness and scarring, while the latter occurs primarily in Black women,” says Dr. Guttman. And as was the case with alopecia areata, there wasn’t much to do in terms of treatment other than immune suppressants or oral antibiotics. “But neither were very effective—and it was devastating for patients,” she says. A recent study at the Alopecia Center published in the American Academy of Dermatology Journal promises an end to that devastation: “We found that JAKs are increased in the scalp of patients with scarring alopecia, and oral JAK inhibitors, if started early enough, can reverse the hair loss. We are now also proving that this may be possible in some cases with topical JAK inhibitors and are going to test topical JAK inhibitors on these conditions, as well. We are very busy with great prospects,” Dr. Guttman says.
A Major NIH-Funded Study Will Explore Treatment for Alopecia Areata in Children
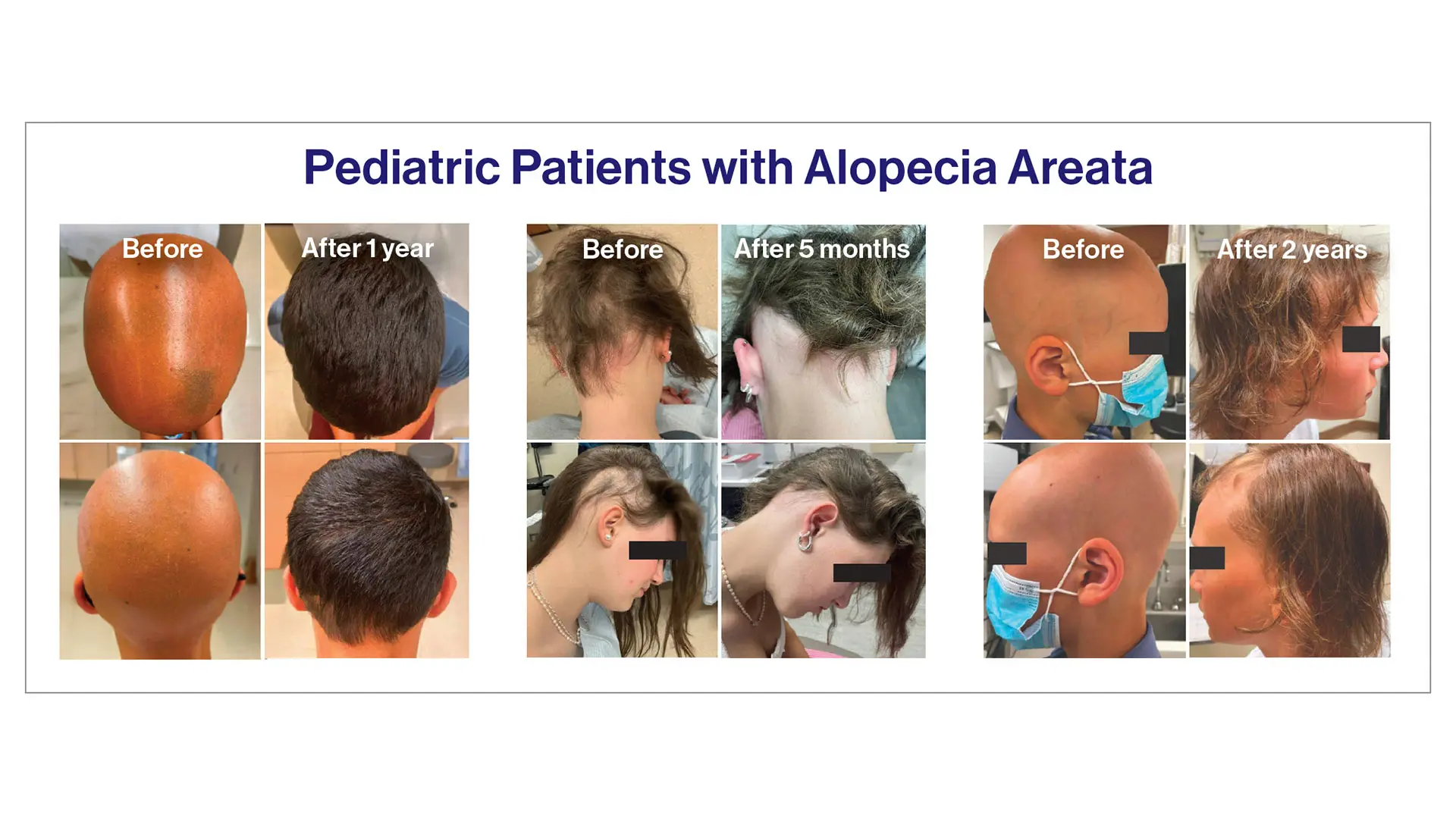
Next on the agenda for the Alopecia Center, thanks to a $6.6 million grant from the National Institutes of Health (NIH): a study of the effectiveness of dupilumab, in children with alopecia areata. Alopecia areata is more common in children than in adults—indeed, 40 percent of patients show symptoms before the age of 20. “Currently, there is only one treatment—a JAK inhibitor known as LitfuloTM— approved for children ages 12 and up. That means children under age 12 have nothing because JAK inhibitors have potential safety concerns,” Dr. Guttman explains. “As a parent, that’s troubling.”
That option—dupilumab—is a monoclonal antibody that has shown strong efficacy and safety, and is already approved for a number of diseases, including atopic dermatitis (eczema) and asthma. Dr. Guttman will lead a controlled trial of 76 children ages 6-17 years old with alopecia areata affecting at least 50 percent of the scalp. These patients will be randomized 2:1 (dupilumab to placebo) for 48 weeks, followed by 48 weeks open-label dupilumab for all participants so everyone can benefit, and lastly 16 weeks follow-up, for a total of 112 weeks.
“With alopecia areata, when you stop using medication, the hair starts falling out again, so we need safe treatments for the long term,” says Dr. Guttman. “The only other available treatment for moderate to severe alopecia areata is JAK inhibitors—and those aren’t approved for patients under age 12. That’s why we are especially excited about testing out this safer option in children.”
First-of-Its-Kind Clinical Trial Aims to Set New Standard- of-Care Protocols for Treating Alopecia Areata and Atopic Dermatitis in People With Down Syndrome
Another exciting study sponsored by the NIH will begin soon, in which individuals 12 years and older with Down syndrome and either alopecia areata or atopic dermatitis will be treated with abrocitinib. Although abrocitinib is approved for atopic dermatitis in the general population for adolescents and adults, it has not been studied specifically in the Down syndrome population. “We are extremely enthusiastic about our upcoming study to evaluate abrocitinib in people with Down syndrome and inflammatory skin diseases,” says Dr. Guttman. “People with Down syndrome have unique systemic inflammation that we believe make them particularly good candidates for this treatment, and we feel fortunate that we will have this opportunity, because usually this population does not have studies that focus entirely on them.”