Using a microaxial flow pump (TV-mAFP) prior to and during cardiac stenting procedures for patients with severe heart attacks who don’t have cardiogenic shock does not significantly reduce heart damage. That is the major finding from the first clinical trial of its kind to analyze the effect of resting the heart in high-risk heart attack patients to see if it reduces the size of the heart attack.
Gregg W. Stone, MD, Professor of Medicine (Cardiology) at the Icahn School of Medicine at Mount Sinai, presented these results from the STEMI-Door to Unload (DTU) trial in March 2026 during a late-breaking clinical trial session at the American College of Cardiology Scientific Session. This work was simultaneously published in the Journal of the American College of Cardiology.
“In medical school we learned that ‘time is muscle’—and during a heart attack, every minute that the artery is not open matters,” says Dr. Stone, the study’s co-principal investigator, Director of Academic Affairs for the Mount Sinai Health System, and Professor of Population Health Science and Policy at the Icahn School of Medicine. “Interventional cardiologists are great at unblocking arteries with stents during this medical emergency, a procedure that saves lives, but we are far less effective at reducing the size of infarct for a variety of reasons. Because of this, many patients have large heart attacks and either don’t survive or develop heart failure.”
Patients who experience ST-segment elevation myocardial infarction (STEMI) require urgent percutaneous coronary intervention (PCI). It is critical to treat these patients as quickly as possible to prevent or limit heart muscle damage, or infarct, especially since STEMI heart attacks can cause cardiogenic shock.
Many strategies have been developed to try to reduce muscle damage during a cardiac stenting procedure, but almost all of them have failed, Dr. Stone says. Only one therapy—supersaturated oxygen—has been shown to reduce infarct size. For decades, experimental studies on STEMI patients both with and without cardiogenic shock have shown that use of a flow pump that ejects, or unloads, blood from the pumping chamber of the heart to the body can rest the heart, improve blood flow to the heart muscle, and, through other complex mechanisms, reduce heart damage.
“While the microaxial flow pump is lifesaving in patients with cardiogenic shock, at the present time we do not recommend its routine use in patients with evolving heart attack without shock.”
Gregg W. Stone, MD
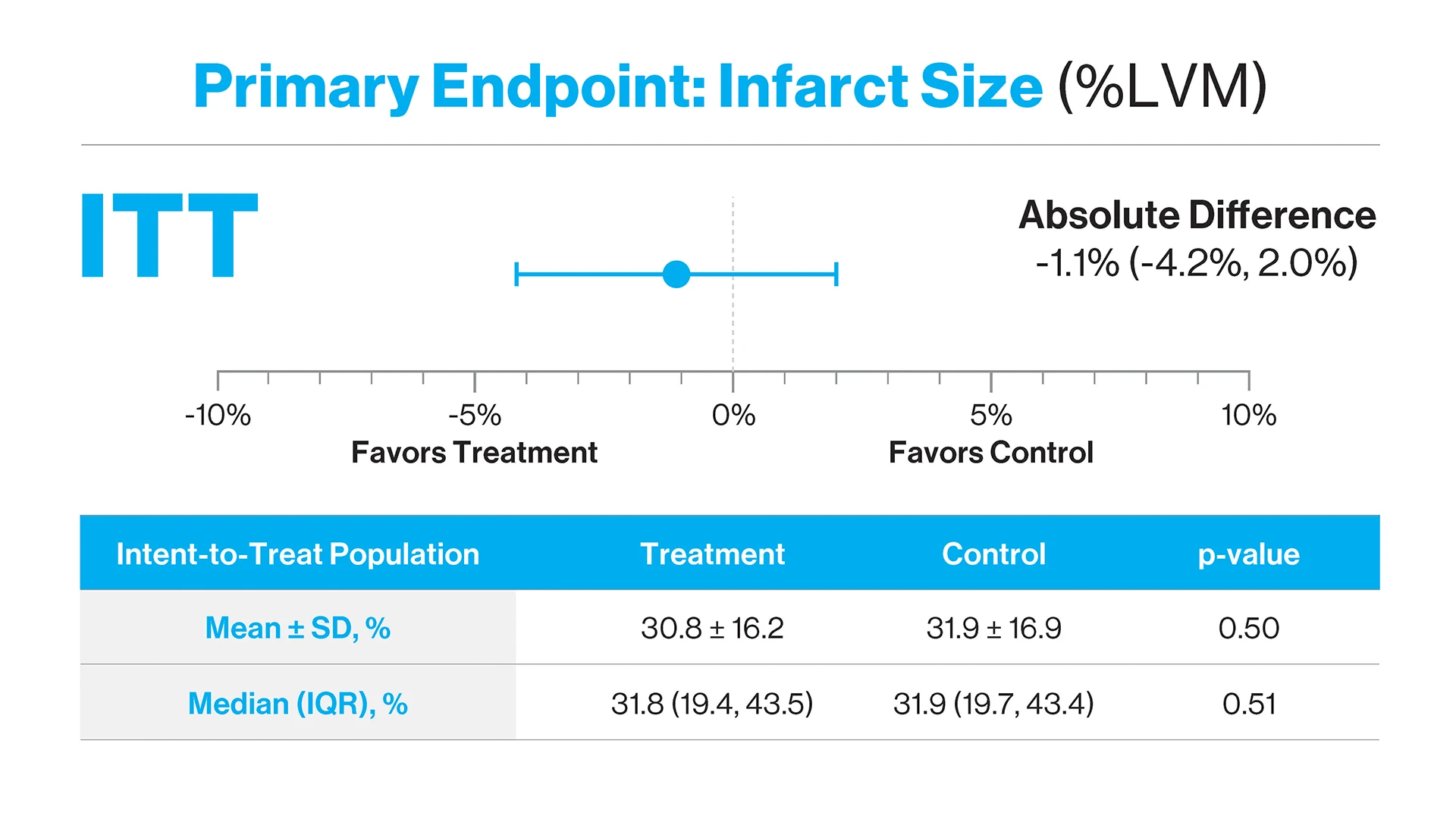
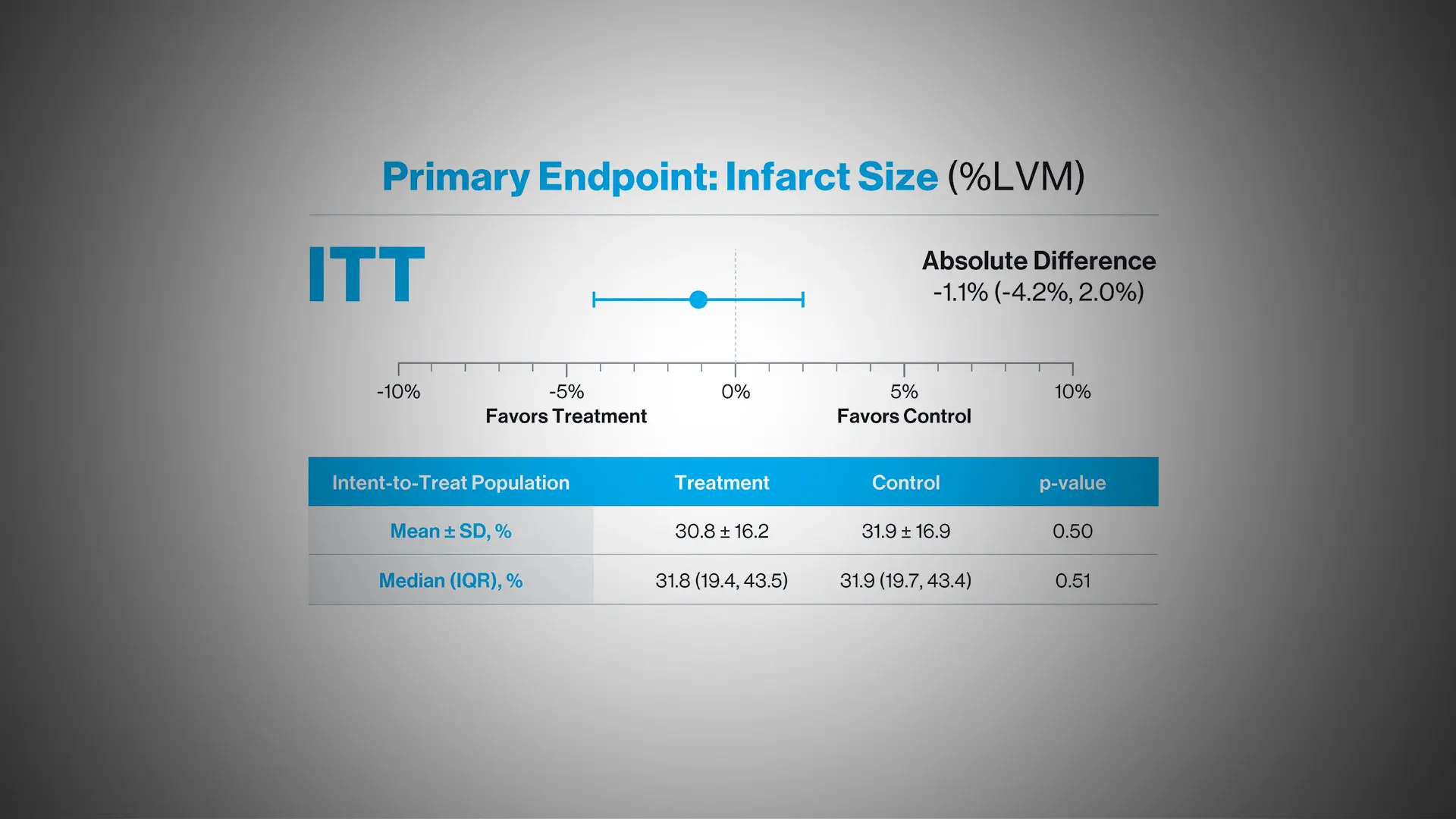
Impella plus delayed PCI did not reduce infarct size compared to the control arm. An absolute reduction of 1.1 percent was observed in the treatment arm. Notably, despite the increase in total ischemic time and delayed PCI, no increase in infarct size was observed. ITT=intention to treat; LVM=left ventricular mass; SD=standard deviation; IQR=interquartile range.
“The DTU trial is the first pivotal trial in 30 years that has tested this hypothesis,” Dr. Stone says. “Unfortunately, infarct size, the primary endpoint of the study, was not reduced, and as expected, there were bleeding complications from the device. Thus, while the microaxial flow pump is lifesaving in patients with cardiogenic shock, at the present time we do not recommend its routine use in patients with evolving heart attack without shock. However, this approach coupled with pharmacologic or other therapies may be synergistic and improve outcomes in high-risk non-shock patients with heart attacks. That is the future direction for new studies.”
The trial focused on the Impella CP device, a Food and Drug Administration-approved catheter-based percutaneous microaxial heart pump manufactured by Abiomed. The researchers investigated the device in patients who had a blocked artery involving the anterior wall of the heart, the location that typically causes large heart attacks, but who were not in shock. In experimental studies, for infarct size to be reduced, the heart pump has to be inserted 30 minutes before PCI. This delays the stenting procedure, which might paradoxically increase the size of the heart attack.
In this study, researchers conducted an open-label, randomized controlled trial at 55 hospitals in the United States, Germany, Italy, the United Kingdom, Switzerland, and Canada. Adults aged 18-85 years with no prior myocardial infarction, presenting with acute anterior STEMI with symptom onset one to six hours before hospital arrival, were eligible for inclusion. Patients were randomly assigned to either left ventricle unloading with the Impella CP for 30 minutes before PCI, or PCI alone.
Between December 12, 2019, and September 3, 2024, 527 patients were randomized; 262 patients were assigned to the treatment group and 265 to the control group. Mean age was 61 ±11 years, and 417 (79.1 percent) were men.
The primary effectiveness endpoint was a reduction in infarct size on a cardiac MRI three to five days after the procedure. The primary safety endpoint was to see if the rate of major bleeding—either device- or procedure-related—or major vascular complications was acceptable if there was a reduction of infarct size.
Infarct size expressed as a percentage of the total left ventricular mass was slightly less in the Impella group compared to the immediate PCI group (mean 30.8 percent ± 16.2 percent vs. 31.9 percent ± 16.9 percent), but this difference did not reach statistical significance. Notably, however, infarct size among Impella patients did not increase despite the delay.
While the trial did not meet its primary endpoint, researchers noted that future studies should build on these findings. “As TV-mAFP technologies and training continue to evolve, which may decrease bleeding risk, the novel findings from the STEMI-DTU pivotal trial set the stage for further clinical investigation to reduce infarct size, attenuate bleeding events, and improve the lives of patients with anterior STEMI,” the study concluded.
Featured
Gregg W. Stone, MD
Professor of Medicine (Cardiology), and Population Health Science and Policy