Although elevated lipoprotein(a), or Lp(a), is a known contributor to atherosclerotic cardiovascular disease, the mechanisms are not well understood. A Mount Sinai team led by Robert S. Rosenson, MD, has advanced the understanding of those processes, implicating tissue factor (TF)—an important regulator of thrombosis. In a series of studies A in 2025, the team made significant progress toward improving the diagnosis and treatment of high Lp(a).
People with early-onset cardiovascular disease often have no idea they are at risk until they experience a cataclysmic event, such as sudden cardiac arrest. Dr. Rosenson, a leading physician-scientist in his field, says he has treated patients in their 20s and 30s who had been resuscitated after cardiac death and found many had elevated levels of Lp(a).
“High lipoprotein(a) is the most common lipoprotein disorder in people with early-onset coronary artery disease,” says Dr. Rosenson, the Rony Shimony Distinguished Professor of Cardiovascular Medicine at the Icahn School of Medicine at Mount Sinai, and Director of Metabolism and Lipids for the Mount Sinai Health System.
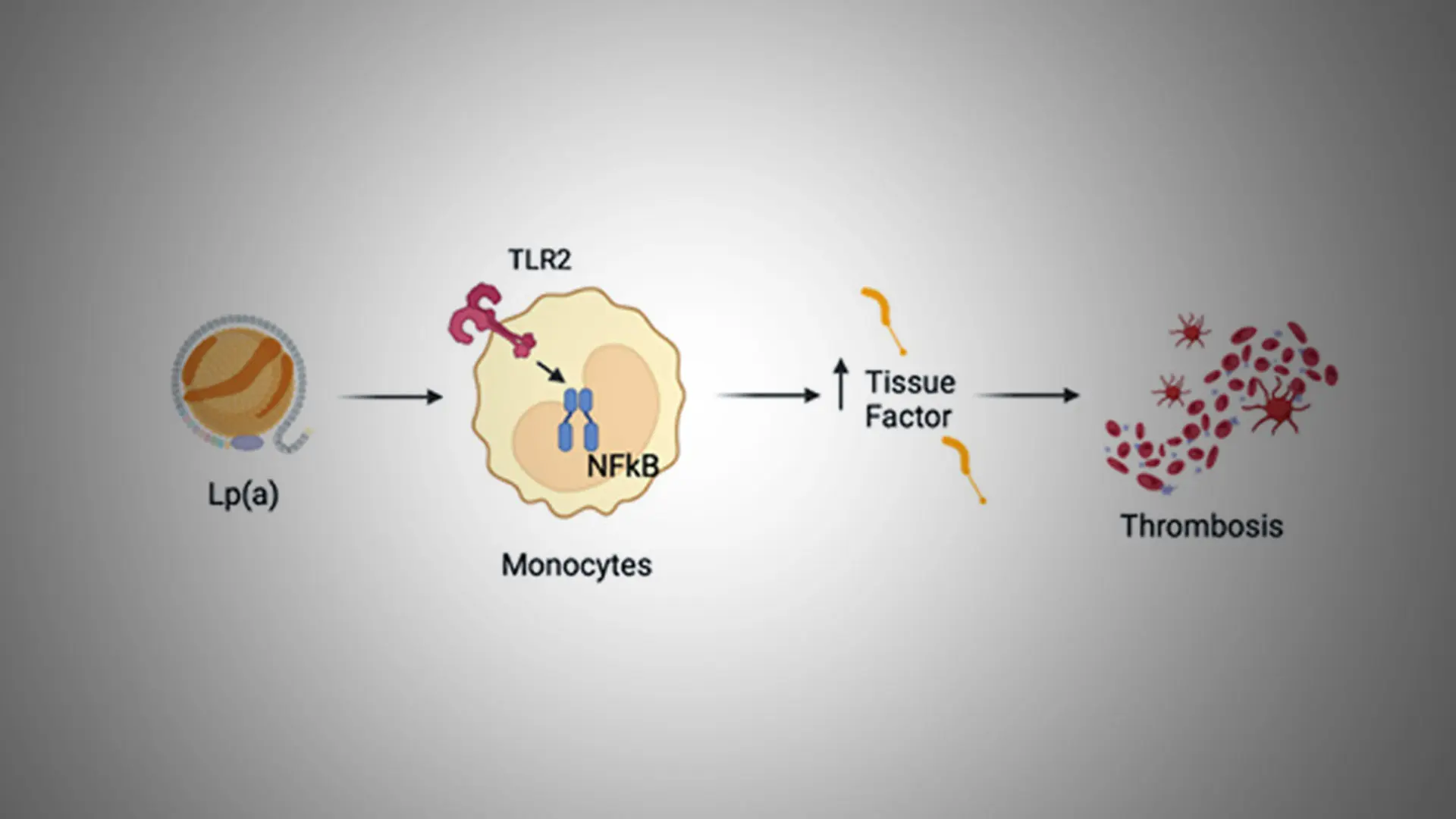
In previous research exploring the link between COVID-19 infections, inflammation, and arterial clotting, Dr. Rosenson and his colleagues identified a role for TF. It is released by macrophages, inflammatory cells that accumulate cholesterol and Lp(a). When macrophages become senescent, they release TF, increasing the risk of a clot when the artery experiences surface erosion or a plaque rupture. “That COVID-19 research made us wonder whether a similar process was happening with high Lp(a),” Dr. Rosenson says.
To find out, his team performed proteomic, transcriptomic, and functional biology analyses on blood samples from 64 patients with atherosclerotic cardiovascular disease. They found striking differences in patients with high versus low Lp(a). Patients with high Lp(a) had significantly higher markers of inflammation and vascular dysfunction, including elevated TF. In addition to more circulating TF, the patients’ mononuclear cells also expressed more TF. Those changes, the research showed, drove the conversion of protein Factor X to Factor Xa—an activated clotting factor that promotes thrombosis. The results were published in the Journal of Lipid Research.
The team has extended the findings to real-world outcomes. Dr. Rosenson and colleagues examined coronary CT angiograms from 525 patients and found that those with high Lp(a) had a different type of plaque than those with high LDL cholesterol. The Lp(a) plaque is less calcified, more lipid-rich, and more likely to rupture. “It’s a whole series of events,” Dr. Rosenson says.
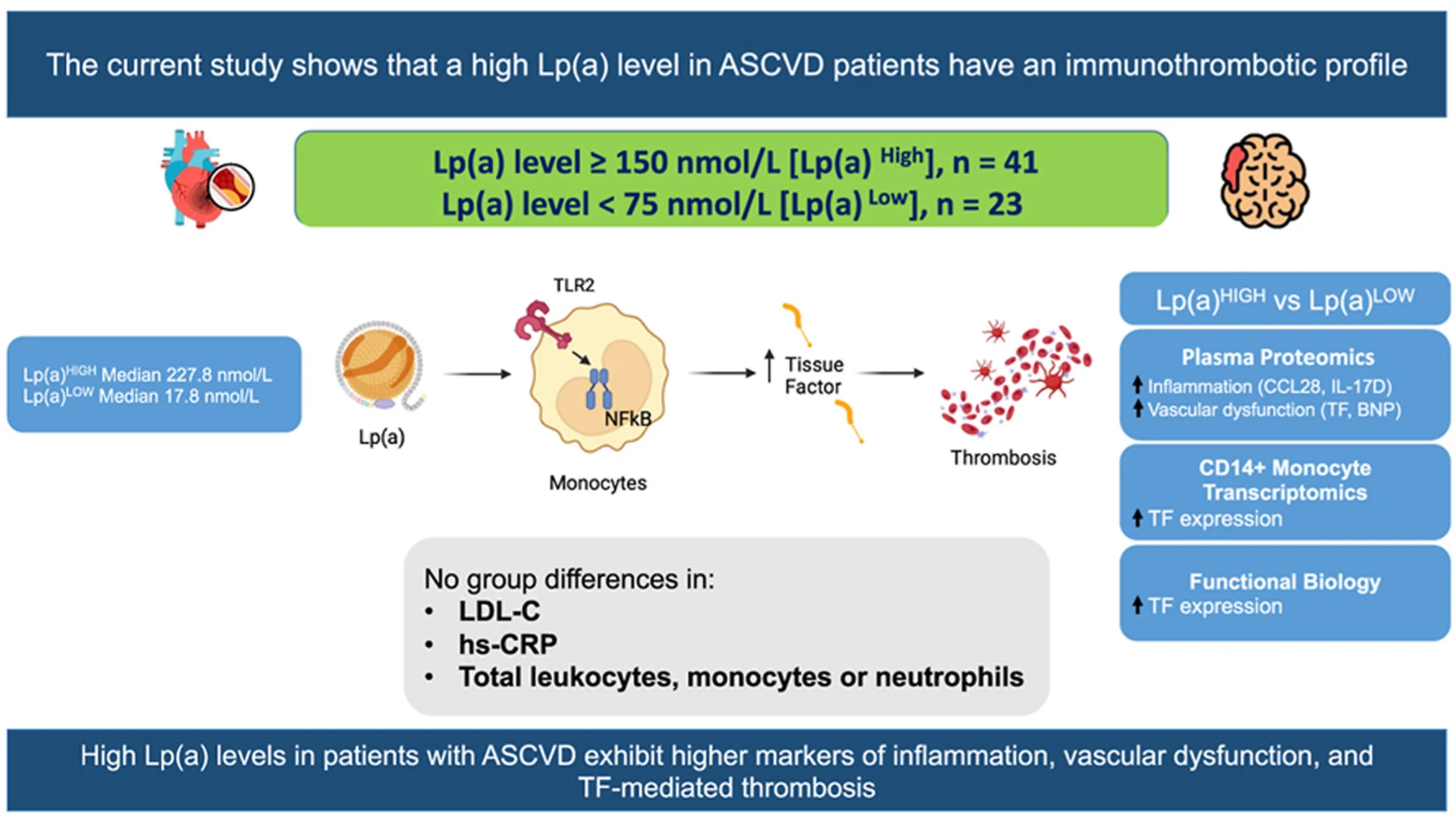
A graphic abstract of the study
“The plaque becomes more likely to rupture, more likely to get inflamed, and then the inflammatory cells release tissue factor. That leads to a big clot that is more resilient and doesn’t dissolve easily.” The findings were presented at the American Heart Association's 2025 Scientific Sessions, and published in January 2026 in the European Heart Journal-Cardiovascular Imaging.
High Lp(a) is largely determined by genetics, and the American Heart Association recommends people have it measured at least once in their lifetime. Yet while as many as one in five people has high Lp(a), not all of them are at increased risk of a cardiac event. “Identifying high-risk patients is far more complicated than just measuring Lp(a),” Dr. Rosenson says.
To learn more, his team turned to samples from participants in the long-running Coronary Artery Risk Development in Young Adults Study (CARDIA). They found that people who had Lp(a) enriched in a TF pathway inhibitor were more likely to experience cardiovascular events than those who did not. Taken together, these studies point to an important pathway by which elevated Lp(a) increases the risk of cardiac events in some, but not all, patients. “It all shows a consistent picture as to why some patients with high Lp(a) have these events,” Dr. Rosenson says.
With this new understanding, the researchers are getting closer to identifying which patients would benefit from treatment. So far, that treatment is imperfect. Statins do not lower Lp(a)—and may even raise it slightly. PCSK9 inhibitors can help, but only lower Lp(a) by about 25 percent, Dr. Rosenson says. New drugs to lower Lp(a) are being investigated in clinical trials—including studies at the Icahn School of Medicine—with early results suggesting reductions in Lp(a) levels as much as 80 to 95 percent or more, Dr. Rosenson notes.
Clarifying the mechanisms of risk in people with high Lp(a) will not only guide treatment decisions but also strengthen clinical trials by helping researchers recruit the right patients—ultimately paving the way for better tools to prevent devastating cardiac events.
“There is a certain unpredictability to Lp(a), but we’re finally getting a better sense of it,” says Dr. Rosenson, who plans to discuss designing better trials for studying Lp(a) in his role as course director for the atherosclerosis sessions at the annual Cardiovascular Clinical Trialists meeting. “These events can be life-ending. Our goal is to identify individuals at risk to get them the attention and care they need.”
Featured

Robert Rosenson, MD
Rony Shimony Distinguished Professor of Cardiovascular Medicine, and Director of Metabolism and Lipids