The current risk- and symptom-based screening tools used to prevent heart attacks fail to identify nearly half of the people who are at risk of having one, according to a retrospective study led by Amir Ahmadi, MD, Clinical Associate Professor of Medicine (Cardiology) at the Icahn School of Medicine at Mount Sinai. The results were published in the Journal of the American College of Cardiology: Advances in November 2025.
The research team assessed the accuracy of the widely used atherosclerotic cardiovascular disease (ASCVD) risk score, and of the PREVENT (Preventing Risk of Cardiovascular Events) tool, a newer measure that adds variables and is intended to provide a more comprehensive estimate of cardiovascular risk along with symptomatic screening.
“Our research shows that population-based risk tools often fail to reflect the true risk for many individual patients,” says Dr. Ahmadi, the corresponding author. “If we had seen these patients just two days before their heart attack, nearly half would not have been recommended for further testing or preventive therapy guided by current risk estimate scores and guidelines. "This study suggests that the current approach of relying on risk scores and symptoms as primary gatekeepers for prevention is not optimal,” Dr. Ahmadi continued. “It may be time to fundamentally reconsider this model and move toward atherosclerosis imaging to identify the silent plaque—early atherosclerosis—before it has a chance to rupture.”
To assess the effectiveness of current screening tools, researchers did a retrospective analysis on data from 474 patients under age 66 with no known coronary artery disease. All patients were treated for their first heart attack at Mount Sinai Morningside and The Mount Sinai Hospital between January 2020 and July 2025. The team collected personal information including patient demographics, medical history, cholesterol levels, blood pressure, and when their symptoms, defined as chest pain or shortness of breath, first appeared. For each patient, the 10-year ASCVD risk was calculated, and a simulated assessment was performed as if the patient had been evaluated two days before their heart attack. Patients were divided into four risk groups: low (under 5 percent), borderline (5-7.5 percent), intermediate (7.5-20 percent) and high (more than 20 percent).

Study authors Amir Ahmadi, MD, and Anna Mueller, MD.
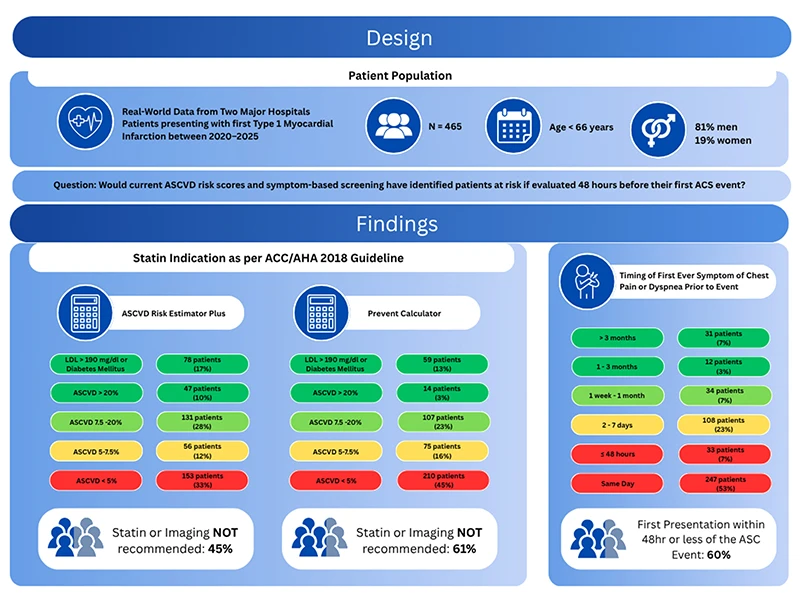
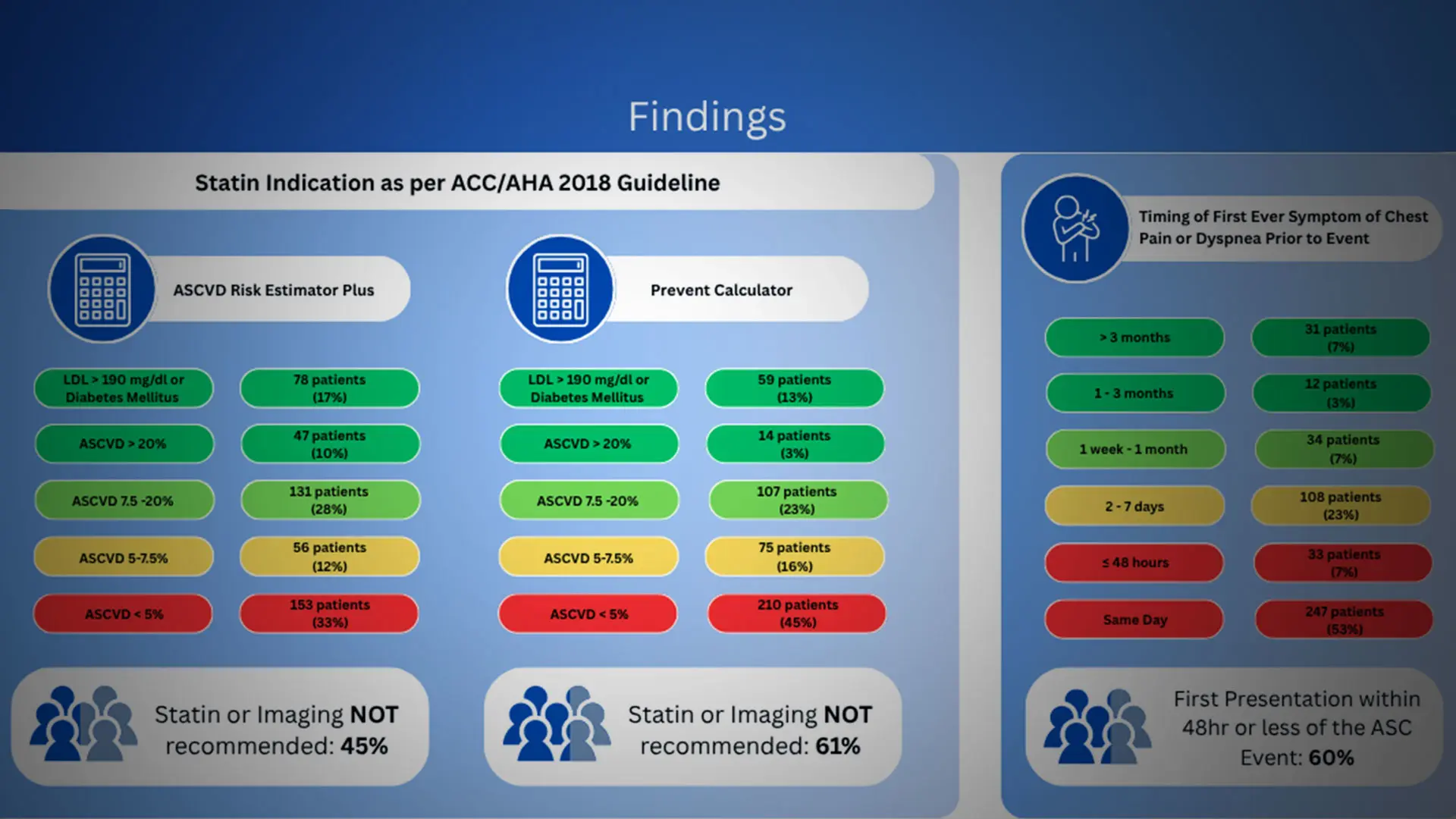
Figure illustrates the distribution of risk categories and symptom timing. Panel A shows classifications based on the ASCVD Risk Estimator Plus, where 45 precent (209/465) of patients would not have qualified for statin therapy or further testing. Panel B displays results from the PREVENT calculator, which classified an even larger proportion—61 percent (285/465)—as low or borderline risk despite subsequent MI. Panel C shows timing of symptom onset, with 279 patients (60 percent) developing symptoms within 48 hours of presentation.
The results focused on two main factors: who would have qualified for preventive treatment based on their risk score, and when symptoms began. Overall, 45 percent of patients would not have been recommended for preventive therapy or diagnostic testing under current ASCVD-based guidelines, and this number increased to 61 percent when using the newer PREVENT calculator. Most patients (60 percent) did not develop symptoms such as chest pain or shortness of breath until less than two days before their cardiac event, showing that symptoms often appear too late to help with changing the course of disease. Together, these findings reveal a critical gap in current prevention strategies: patients who appear healthy by standard measures may already have significant, silent heart disease. Relying solely on risk scores and symptoms delays diagnosis until it is too late for prevention.
“When we look at heart attacks and trace them backward, most heart attacks occur in patients in the low or intermediate risk groups. This study highlights that a lower risk score, along with not having classic heart attack symptoms like chest pain or shortness of breath, which is common, is no guarantee of safety on an individual level,” says first author Anna Mueller, MD, an internal medicine resident at the Icahn School of Medicine. “Our study exposes a major flaw where tools effective for tracking large populations fall short when guiding individualized care. Instead, doctors should shift their focus from detecting symptomatic heart disease to detecting the plaque itself for earlier treatment, which could save lives.”
Researchers say more studies are needed to further this work, and future research should focus on optimizing strategies to enhance early detection and prevention, including cardiovascular imaging.